

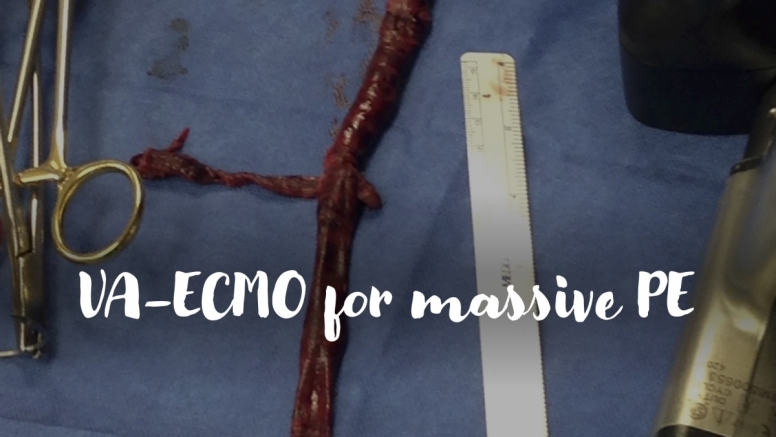
A 60-year-old man presents to the ED after an episode of syncope. He is initially hemodynamically stable and undergoes CT demonstrating saddle pulmonary embolism. He returns from radiology with tachycardia and hypotension refractory to fluids and requiring vasopressor support. Bedside echo reveals RV dilation and severely reduced RV systolic dysfunction with septal flattening consistent with RV pressure overload. As you start systemic anticoagulation with heparin, you consider the indications for thrombolysis, surgical embolectomy and VA-ECMO.
Read moreSubmitted by Emily Damuth, MD

Do you know which substances in YOUR house are capable of causing debilitating tissue injury if ingested?
Read moreSubmitted by Alyse Volino, MD

A 40 yo female presents with knee pain
Read more
Submitted by Sandhya Ashokkumar, MD


What exactly is drowning? What do we need to worry about in drowning injuries? How do we manage them in the ED?
Read more
EMS calls ahead with reports of an adult patient in respiratory distress. They are concerned the patient will need to be intubated on arrival. Recognizing the name, you pull up a previous chart and review the patient’s history. You realize this is their 10th presentation this year and on reviewing their most recent oncology note you note their oncologist has recommended they consider hospice due to end stage malignancy without further treatment options. The patient arrives, is in distress, and does not have capacity but can be temporized by NIPPV while decision making occurs. Their power of attorney comes to the hospital soon after but states they never got around to establishing an advanced directive. How should you approach this conversation?
Read moreSubmitted by Lars-Kristofer Peterson, MD

Question: Is point of care ultrasound (POCUS) in the ED as accurate as CT for diagnosing small bowel obstruction (SBO)?
Read moreSubmitted by Eric Chavis, MD